Nearly three years ago my husband had Total Knee Replacement (TKR) surgery. It’s drastic and major surgery, which people usually only choose when the pain from osteoarthritis becomes intolerable. And, it was not done properly so that last month it had to be re-done! Perhaps our experience can be useful to others.
Why do knees need to be replaced?
Generally because of pain and restricted motion caused by loss of cartilage (which cushions and separates the bony parts of a joint) and growth of bony “spurs”. This is labelled osteoarthritis. Other causes, like trauma, rheumatoid arthritis, and infection, account for a minority of the 300,000+ TKRs each year in the US.
As to what causes osteoarthritis, that is less understood than previously thought, when it was all blamed on “wear and tear”. The knee is the largest joint in the body, and bears the complete weight of the body at each step we take, so it is indeed subject to lots of “wear and tear”. Common-sense risk factors include types of high-stress activity in work or sports, injury, obesity, infection, stiffness from lack of activity, and age (since cartilage becomes more brittle with age). However, not all elderly people develop arthritis and some who do have no significant pain. This is why I said above that knees need to be replaced, not because of osteoarthritis, but because of pain and reduced range of motion.
The biologic factors leading to the deterioration of cartilage in osteoarthritis are not entirely understood. Many experts believe that osteoarthritis results from a genetic susceptibility that causes some biologic response to injuries to the joint, which in turn leads to progressive deterioration of cartilage. In addition, the ability to make repairs becomes progressively limited as cartilage cells age.
Although osteoarthritis generally accompanies aging, osteoarthritic cartilage is chemically different from normal aged cartilage. As chondrocytes (the cells that make up cartilage) age, they lose their ability to make repairs and produce more cartilage. This process may play an important role in the development and progression of osteoarthritis. [Emphasis mine. Source: www.healthcentral.com ]
What’s involved in Total Knee Replacement surgery?
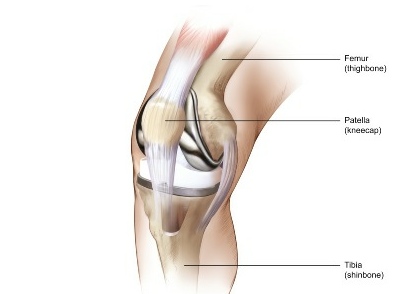
The x-rays below, from the site of a prosthetics manufacturer,
show views of a knee before and after surgery. On the left, cartilage loss has caused bone-on-bone contact: very painful. Bone spurs or bits of broken bone floating around can also cause pain in the deteriorated joint. On the right, an artificial knee joint (prosthesis) is in place. (These are not x-rays of the same knee; in fact, looks to me like one’s a left leg and the other is a right leg.)
Here are some views of prostheses. To install them, the ends of the two long-bones of the leg, tibia and femur, are sawed off (removing “usually between 2 and 12 mm” according to one source) and the artificial joint is affixed with cement, screws, etc. The work involved in removing bone and attaching the prosthesis involves considerable force and power tools. Note that the knee-cap, as well as muscles and ligaments, must be carefully moved aside to install the prosthesis. [Picture sources: 1, 2, 3 ]


There are many patented designs for artificial knee joints, and these illustrations are for general example only. Surgeons have their preferred models; many were developed by orthopedic surgeons, and those surgeons tend to prefer the ones they have an interest in. Choice of prosthesis isn’t something the patient can weigh in on, we don’t know enough, but you may want to find out if your surgeon has a financial interest in the one he is going to use; if so, perhaps a second opinion would be valuable on the pros and cons of various types as applied to your individual case. Most insurance will pay for a second opinion for major surgery.
Research continues for better, longer-lasting designs and breakthroughs are regularly announced with fanfare––but some don’t fulfill their original promise, as with teflon-lined joints which wore away much faster in practice than lab tests had predicted. You will have to rely on the experience of your surgeon.
You can see photos of the stages of knee surgery (not for the faint-hearted) here, on a prosthesis company ‘s site.
Our experience
Surgery #1, 2006
Now, back to my husband’s case. Dan had knee pain for years that ruled out unnecessary walking, as in hiking or walking for enjoyment, and interfered with sleep. There was bone on bone contact and perhaps bone spurs or growths from osteoarthritis. In August 2006 he underwent total knee replacement surgery by an established older orthopedist in our area. Afterwards, the surgeon came out to me in the waiting room and told me that the operation had taken half again as long as planned because they had “run into something unexpected”. Later, when we knew more, that remark would have much more significance to us. The “something unexpected” was apparently the result of a broken leg at age ten, that had caused greater reliance on the other leg (the one that received the TKR).
The surgery was brutal, with terrible bruising all over the leg, and post-op pain and swelling were severe. From the beginning, the prosthesis felt loose and insecure, sometimes the knee buckled, and after the post-surgical pain subsided, he was still in pain sufficient to make walking difficult. At each visit with the surgeon Dan raised these issues and was told to exercise more, and that it would get better with time. Two years on, that hadn’t happened, and the surgeon then agreed that the knee was a bit loose and offered to go back in and “put a shim in it”.
At some point after the 2006 operation, when it became apparent that it had been unsuccessful, I began to research the subject. Immediately I found that it’s common practice now to use Magnetic Resonance Imaging before TKR, rather than merely relying on x-rays. MRIs provide an exact and minutely detailed three-dimensional picture of the joint. The data can be used to make a 3-D visualization that can be rotated. This way the surgeon knows exactly what to expect; the prosthesis is customized, if necessary, beforehand; the surgery is generally shorter and the incision may even be smaller. (Other advances, such as computer-assisted orientation systems to guide the surgeon in positioning the prosthesis during surgery, may also be used.) Nothing like this was done in Dan’s case, and we didn’t know to ask about it. We know now that the original surgeon does have access to an MRI, in the hospital across the street from his office, and used it to look at Dan’s hip after the bad artificial knee began to cause a lot of pain in his hip, back, and other knee. But he didn’t use it for the knee needing replacement.
Surgery #2, 2009
Finally, after the remark about putting in a “shim”, we began to look for another surgeon. I searched online for someone who used MRIs and computerized techniques for joint replacement and who was experienced in what I learned is called “revision” (re-do) of TKRs. (Some surgeons, including the only other ones in our area, won’t touch someone else’s failures.) I found a surgeon who met these qualifications, about 4 hours drive from where we live, and we went to see him. The first thing he did was to get a full-leg digital x-ray, which surgeon #1 had never done. He showed us the x-ray, and used software to examine the precise alignment of the prosthesis. It was 7.5° out of alignment. In effect, his lower leg-bone had been detached and then put back on at a different angle from the upper leg. For over two years the first surgeon had taken no steps to examine the results of his surgery, other than feeling the knee.
We liked what we saw here, added to what we already knew about Surgeon #2’s experience, and proceeded with the preparations for a revision.
In late May Dan went through the revision surgery. Pry off the old, shave off a little more bone, affix the new.
When the surgeon met with me afterward in the waiting room, he had troubling things to report but they weren’t about what had just taken place. He told me that the prosthesis he had removed was badly installed. He actually used the word “sloppy”––and you know how rare it is for doctors to criticize one another’s work! The lower part was out of alignment both front-to-back and side-to-side; the upper part was supposed to be stabilized by the bone growing into it on all sides, but this had not taken place (he remarked that he did not use this model because sufficient bone regrowth often failed to occur). So this artificial joint had been loose and seriously mis-aligned, with every step stressing both parts of the prosthesis, the ends of the bones, the muscles/ligaments/tendons, and the other joints involved in walking (back, hip, other knee). It was clear, said the surgeon, that this had been causing Dan considerable pain, and he felt confident that the new prosthesis was going to be a great improvement.
Today is post-op day 19, and there is no comparison between the two post-op experiences. The day after the surgery they got Dan on his feet, and the first time he put his weight on the new knee he said that it felt more solid than the old one ever had. The next day he was walking the hall, slowly, and walking without hip pain for the first time in ten years. Bruising of the leg is minimal, the incision is shorter, and pain is less. The first time he was using fentanyl patches, very heavy opioid painkiller, and was still in too much pain. This time it is Tylenol-3 every 4 hours, and ultram (tramodol) occasionally when needed.
The incision is closed with superglue, covered with crossways lengths of what looks like strapping tape: no staples to distort the skin and then have to be removed. He was able to take a short shower on post-op day 5. Last time the first shower was not permitted nearly so soon and he was in so much pain he had to sit down on a plastic bench in the shower. This time, he was easily able to stand and feel secure. He’s in pain, but not nearly as much as last time, and the solidity of the knee makes it possible for him to get around the house carefully but confidently, only occasionally using his walking stick for stability (and to keep the dogs from bumping him).
Like the first time, the anesthesia was a spinal block (not general anesthesia) but the new surgeon added a femoral nerve block. As I understand it, the spinal keeps pain messages from reaching the brain during surgery; the femoral block keeps the nerves immediately affected by the surgery from registering pain which gets the nerves excited even though the brain doesn’t hear about it. It’s supposed to lessen post-op pain and it certainly seems to do that, especially for the first 24-36 hours.
There is swelling, but it’s not bad unless he keeps his leg bent too long while sitting; last time he was still mostly in bed for at least 2 weeks, and the swelling was severe from above the knee to the foot. Perhaps this is related to another difference in surgical procedure: this time a drain was placed near the incision with a receptacle attached which had to be periodically emptied of fluid, partly blood. Before the drain was removed, 1200 cc of fluid had been collected. The first surgeon did not place such a drain, the leg continued very swollen, and at the two-week check-up the surgeon had to use a syringe to remove at least 200 cc from the still very swollen knee. Doing this is risky because in raises the risk of infection, which would be a dire complication.
At this point the future looks very good for this new knee, and we are talking about being able to get out and hike with our dogs again. I still have limited energy (fibromyalgia) but more than I used to, since getting off of methadone which I took for pain.
Lessons learned
The parts of our experience that I think may be useful to everybody facing joint replacement surgery are these:
Research and ask questions. Get a second opinion.
This is major surgery which will shape your everyday life for the next decade or more. Revisions are to be avoided: not only because of pain and expense, but each surgery removes a little more bone. Don’t be afraid of getting a second opinion, even if your orthopedic surgeon seems great. Believe me, if your orthopedist were going in for brain or heart surgery, he or she would ask around, not just take the first name in the phone book! Insurance generally covers second opinions for major surgery.
Educate yourself about the surgery in general: what can go wrong, and why? what are the different methods?
In choosing a surgeon, standard advice is to find someone who has done this particular surgery a lot and does it regularly. That’s good advice, but incomplete. Our first surgeon had lots of experience and he performs knee replacements regularly. But based on results and what we’ve learned since, this fellow has not kept up with new methods: MRI’s, femoral nerve blocks, post-surgical drains, etc.
Of course nothing is better just because it is new. Some things provide an advantage even the layperson can evaluate, such as the use of MRI’s to see exactly what the joint and surrounding bone look like, so that the operation can be planned using that information. There’s no real downside for the patient in providing better information to the person doing the cutting and sawing. As for the high-tech implantable prostheses used in TKR, there’s always something new coming out, which may or may not be better. You can at least ask a surgeon how long he has been using the device he intends to implant into your body, what the failure rate is, and when and why it fails. Does it fail to be stabilized by bone growth, or do components or surfaces wear out? Does it loosen in 2 – 5 years, for whatever reason? Do particles get ground off and act like grit in a bearing?
Read up on the subject and you’ll get an idea of what to ask. Take notes on your reading and your concerns, and bring them with you; then take notes on what the doctor says. Have someone else come along to help by writing things down, reminding you of questions, and in general giving you moral support. The doctor is the expert, but your body is what’s at risk; don’t be timid about asking. In my mind, a doctor who won’t answer my questions fully, as fully as I want, doesn’t get my business.
Also ask what to expect after the surgery. Surgeon #1 kept stringing us along, telling us that things would get much better. Now we hear from others that isn’t really true, that you “know” right away. And indeed the bad job felt loose from Day 1 and never changed; the recent revision felt solid from Day 1. Certainly, telling us for 2 years that there would still be improvement, was unrealistic (charitable interpretation) and dishonest (blunt interpretation).
More information on Total Knee Replacement
There’s an encyclopedia-style summary of the procedure, risks, failures, etc. here that looked good to me, and another page on this site deals with TKR revisions (re-doing the TKR).
Wikipedia also has good information.
How to reduce the chances that you’ll need knee replacement surgery
It’s no fun, really. And you’ll get stopped by airport security for a special check, every time.
Photo from Wikimedia Commons.
Here’s the advice from the National Institutes of Health––
How Can People Prevent Knee Problems?
Some knee problems, such as those resulting from an accident, cannot be foreseen or prevented. However, people can prevent many knee problems by following these suggestions:
Before exercising or participating in sports, warm up by walking or riding a stationary bicycle, then do stretches. Stretching the muscles in the front of the thigh (quadriceps) and back of the thigh (hamstrings) reduces tension on the tendons and relieves pressure on the knee during activity.
Strengthen the leg muscles by doing specific exercises (for example, by walking up stairs or hills or by riding a stationary bicycle). A supervised workout with weights is another way to strengthen the leg muscles that support the knee.
Avoid sudden changes in the intensity of exercise. Increase the force or duration of activity gradually.
Wear shoes that fit properly and are in good condition. This will help maintain balance and leg alignment when walking or running. Flat feet or overpronated feet (feet that roll inward) can cause knee problems. People can often reduce some of these problems by wearing special shoe inserts (orthotics).
Maintain a healthy weight to reduce stress on the knee. Obesity increases the risk of osteoarthritis of the knee.
What Types of Exercise Are Best for People With Knee Problems?
Ideally, everyone should get three types of exercise regularly:
Range-of-motion exercises to help maintain normal joint movement and relieve stiffness.
Strengthening exercises to help keep or increase muscle strength. Keeping muscles strong with exercises – such as walking up stairs, doing leg lifts or dips, or riding a stationary bicycle – helps support and protect the knee.
Aerobic or endurance exercises to improve function of the heart and circulation and to help control weight. Weight control can be important to people who have arthritis because extra weight puts pressure on many joints. Some studies show that aerobic exercise can reduce inflammation in some joints.
If you already have knee problems, your doctor or physical therapist can help with a plan of exercise that will help the knee(s) without increasing the risk of injury or further damage. As a general rule, you should choose gentle exercises such as swimming, aquatic exercise, or walking rather than jarring exercises such as jogging or high-impact aerobics.
So there it is, same old thing: exercise and lose weight. If you really really do not want a titanium and plastic knee, losing weight is probably the best thing you can do. “Data from the first National Health and Nutrition Examination Survey (HANES I) indicated that obese women had nearly 4 times the risk of knee osteoarthritis as compared with non-obese women; for obese men, the risk was nearly 5 times greater.” Moreover, if you already have knee pain, losing even ten pounds can significantly reduce both pain and the ongoing deterioration of the knee. Being only 10 pounds overweight increases the force on the knee by 30-60 pounds with each step. You don’t need to reach your ideal weight; any reduction will help. And maybe that will be encouragement enough to keep going, slowly, losing weight and feeling better. (Thorough discussion of weight loss and osteoarthritis, here.)





{kind=link}
{kind=link}